Table Of Content
The simple parallel cluster trial achieves the highest level of power when the intra-cluster correlation is small (0.01). However, when the intra-cluster correlation is large (0.1) the power available under the simple parallel design drops to just 50%, while the power available under both the parallel design with a baseline period and the stepped wedge design (with four steps) retains a value close to 80%. In this example, the power under the stepped wedge cluster trial is only slightly larger than that under the parallel cluster trial with a baseline period.
Brief history of the stepped wedge cluster randomised trial
Grand Rounds December 1, 2023: Guidelines for Design and Analysis of Stepped-Wedge Trials (James P. Hughes, PhD) - Rethinking Clinical Trials
Grand Rounds December 1, 2023: Guidelines for Design and Analysis of Stepped-Wedge Trials (James P. Hughes, PhD).
Posted: Wed, 06 Dec 2023 08:00:00 GMT [source]
We developed a framework and terminology by which to define the key characteristics of an SWT and the cluster allocation. We then developed a typology of individual exposure and measurement, and with that in mind, examined the recently published SWTs reviewed in this series [1] to identify commonly used designs and illustrative case studies. We considered the strengths and weaknesses of the commonly used designs, focussing on the possibility of carry-over effects. The work presented here did not require ethical approval as it involves only critical thinking and review of published research articles.
METHODS:
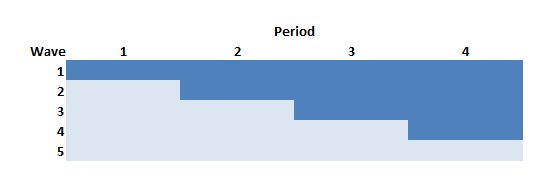
In a stepped wedge design, an intervention is rolled-out sequentially to the trial participants (either as individuals or clusters of individuals) over a number of time periods. The order in which the different individuals or clusters receive the intervention is determined at random and, by the end of the random allocation, all individuals or groups will have received the intervention. Stepped wedge designs incorporate data collection at each point where a new group (step) receives the intervention.

The stepped wedge trial design: a systematic review
It would appear that focussing data collection on the rollout period, and perhaps extending the rollout period, would have provided a more informative trial. The collection of extensive data after the rollout period did, however, permit a per-protocol analysis. Conversely, in case study two it seems that since outcome data are routinely collected that data from immediately before the rollout period could have been compiled and included in analysis if the participants attended the same school before the year of the trial. We recommend that the design of an SWT should be described in terms of how individuals are exposed, including the start and duration of exposure, and whether some, all, or no individuals experience both the control and intervention, and how outcome measurements are obtained.
The intervention was based on a similar intervention that had been hailed as reducing intensive care infections by 80% in a non-randomised, before and after design in Michigan. Formal methods for sample size and power calculations have been described only for cross-sectional stepped wedge designs.4 13 For this reason, a cross-sectional study is assumed throughout the following paragraphs. Similar considerations apply to cohort designs, but a reliable sample size algorithm for these designs has not yet been established. This design (with the addition that control clusters received the intervention at the end of the study) was used for the evaluation of the Mexican Universal Health Insurance Programme, described in example 2.
Have to be estimated as part of the analysis of an SWD trial, the trial is usually (4) planned as described above for settings in which s2 and ? Using these conditions, the standard error (stderr) of the optimum estimator of the treatment effect can be calculated exactly. A relatively simple formula can be used (Box 1) to do so for arbitrary numbers of intervention start times (T) and clusters (n) that transition from the control phase to the intervention phase at the same time. This formula can be used to calculate a confidence interval for the estimated treatment effect obtained by analyzing an SWD trial.
The facts and conclusions on statistical planning and analysis of SWD trials that are summarized here hold under the assumption that both the variance s2 between clusters and the correlation coefficient ? Whenever an SWD trial needs to be analyzed without this prior knowledge, a much more complicated statistical procedure must be used allowing to estimate in addition to the treatment effect ? SWD trials were described in the literature on experimental design as early as the late 1970s (2).
Two approaches taken to reduce both of these problems are matching and stratification [17]. Both approaches potentially reduce the between-cluster variation and improve balance and must be taken account of in the analysis. Stratification can also be used in the randomisation of the order of cluster rollout for an SWT. If clusters are divided into strata, the order of rollout can be randomised within each stratum.
It is more common to use cross-sectional sampling of individuals at pre-specified times to provide data on the outcome of interest. In other settings where clusters are large (such as cities), then only a very small proportion of participants are sampled for outcome measurement at each time, so individuals are measured once at most. Compared to parallel CRTs, SW-CRTs require more sophisticated statistical considerations for design and analysis. In this review, we explore current state of methodological developments for stepped wedge designs and reflect upon potential opportunities for their adoption in neurosurgery trials. These properties are illustrated in table 1⇓, which shows how power depends on the intra-cluster correlation in a cross-sectional study. The example uses the method of Hussey and Hughes4 13 and refers to a trial with 20 clusters and total cluster size of 50 designed to detect a standardised effect size of 0.3 (at 5% significance).
The methodological descriptions of stepped wedge studies, including methods of randomisation, sample size calculations and methods of analysis, are not always complete. Sometimes there is a lag period between when a cluster crosses over and when the intervention can affect the outcome in individuals. This may arise from a combination of implementation lag (delay until the intervention is fully implemented) and delay for the outcome to respond to the intervention. In open or closed cohort SWTs, the step length may be chosen so that the effect of the intervention in the group of clusters that most recently crossed over can be measured just before the next crossover point; therefore the length needs to be greater than the lag period. Delay for the outcome to respond is not relevant for the short exposure continuous recruitment design, as individual follow-up may be long and its length is unrelated to the steps.
In the supplementary table of our review [1], each SWT is assigned to one of these three designs, aside from two trials following non-standard designs described later. Extra variation and limited df always reduce power, so it is essential to consider these factors while the study is being planned, and particularly as part of the estimation of sample size. There are two key (non-exclusive) situations in which a stepped wedge design is considered advantageous when compared to a traditional parallel design. First, if there is a prior belief that the intervention will do more good than harm [5], rather than a prior belief of equipoise [6], it may be unethical to withhold the intervention from a proportion of the participants, or to withdraw the intervention as would occur in a cross-over design.
Typically, study participants are randomly allotted in clusters to the different treatment options. In the parallel GRT, the groups or clusters in the control condition remain in that condition throughout the trial. As such, if external events occur that affect the outcome, that will be seen in the control condition and it may be possible to adjust for it. In the SWGRT, the groups or clusters gradually cross over from the control condition to the intervention condition, so that there are fewer and fewer groups or clusters in the control condition as the study progresses. That can make it difficult to observe or adjust for the effect of an external event that may affect the outcome. In the heterogeneous intervention effect setting, the intervention effect changes with time, requiring greater care in defining the estimand of interest.
This paper presents a review of 12 studies (or protocols) that use (or plan to use) a stepped wedge design. One aim of the review is to highlight the potential for the stepped wedge design, given its infrequent use to date. The stepped wedge cluster randomised controlled trial is a relatively new study design that is increasing in popularity. It is an alternative to parallel cluster trial designs, which are commonly used for the evaluation of service delivery or policy interventions delivered at the level of the cluster. The design includes an initial period in which no clusters are exposed to the intervention. Subsequently, at regular intervals (the “steps”) one cluster (or a group of clusters) is randomised to cross from the control to the intervention under evaluation.
In these trials, a neurosurgeon or a service unit performing neurosurgical operations was the unit of randomization, and the study intervention program often aimed at improving surgery-related patient care. Furthermore, the advantage of rolling out the intervention to all clusters and logistical convenience in staggered implementation were the primary reasons for choosing a stepped wedge design. Following these published trials, when limited resource or capacity is available to simultaneously roll out the program in a future neurosurgery trial, a SW-CRT may be considered as a robust design to effectively study intervention programs. In addition, three trials in Table 3 included fewer than 10 clusters, in which case a stepped wedge design can be more powerful than the parallel-arm design by leveraging both within-cluster and between-cluster comparisons.
Kork-Ease, founded in Brooklyn in 1953, has been a go-to brand for platform wedge sandals. It has since updated some of its bestselling classics, like the Ava, to be even more comfortable and supportive. This pair has a high-quality leather upper that softens over time and an inner foam system designed to cushion the foot with lightweight airiness. The cork footbed is naturally odor-resistant and will mold to your foot’s shape, giving you a customized fit.
Reasons for the secular trend are probably multifaceted and include, but are not limited to, a rising tide of activities directed at improving patient safety and the contamination of the intervention in clusters waiting to be crossed over. Four of the studies [4, 12, 19, 21] included long term follow-up beyond the period in which stepping took place, since the outcomes to be assessed may occur at a point following the final step (i.e. there is a lag between intervention and outcome). Ethics alone was not the presiding consideration for grantees selecting the SW-CRT design. As noted, 3 cooperatives selected alternate designs that allotted delivery of the intervention to all practices. Joag et al reported that the strongest arguments for selecting SW-CRT design are often political and logistical rather than ethical.16 As was the case in the present study, SW-CRT design was recommended by the funder, which might have affected grantees’ design selection.







No comments:
Post a Comment